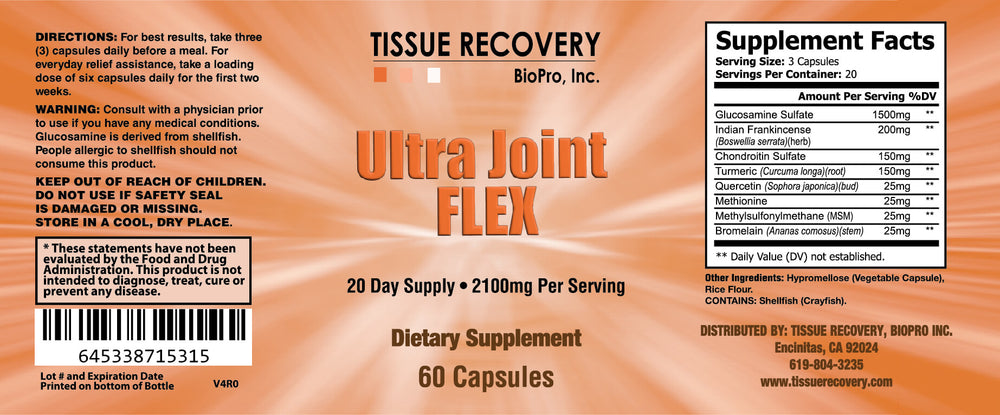
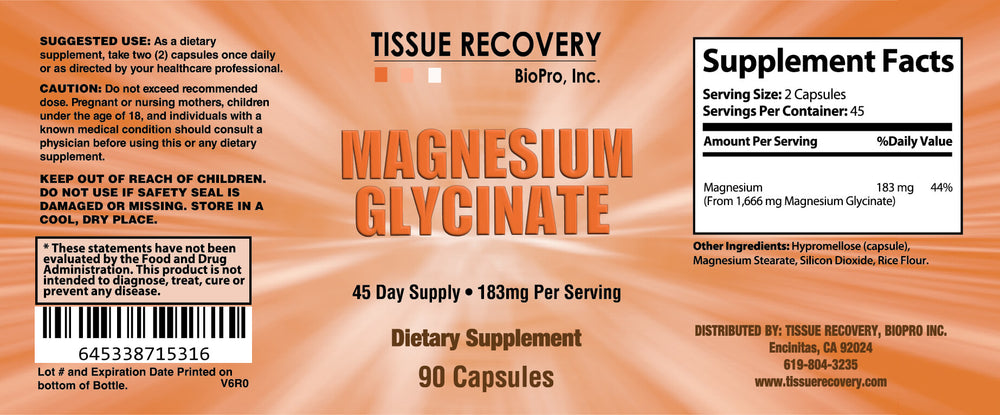
We have replaced the BMJ formula with Ultra Joint Flex and Magnesium Glycinate focusing on joint health. We suggest that you take these two formulas together to achieve the best results, they can however also be ordered separately.
This is what Robert S. Hoffman, M.D. says about the BMJ:
I take the BMJ formula myself, and I recommend it to my patients.
The BMJ provides multiple nutrients in a very bioavailable form with benefits documented by research. Bone Included is patented dicalcium malate for improved calcium bioavailability. See the comparison graph. A (Blue-Dicalcium Malate, Red-Calcium Carbonate)
Excerpted and summarized from the full study entitled Comparison of calcium Absorption from various calcium-containing products in Healthy Human Adults: A Bioavailability study. Copyrights, Albion International, Inc. November 2005
Calcium is important, but it is not necessary to take high amounts according to research. When a two-year study compared perimenopausal women who took either 1000 mg or 2000 mg of calcium daily with a placebo group, the groups taking calcium increased their bone density by 1.6%. No difference was found between the groups taking 1000 mg or 2000 mg indicating there is no reason to take high amounts (Elders PJ, et al. 1994). Bone also needs other important nutrients. Magnesium has shown to prevent fractures and increase bone density (Sojka JE, Weaver CM. 1995, Stendig-Lindberg G, et al. 1993). Bone density has been found to be significantly better when the minerals zinc, copper, manganese, and potassium were added to calcium (Strause L, et al. 1994). Zinc intake and plasma zinc concentrations have been documented to be lower in men with osteoporosis, this has also been reported for women (Hyun TH, et al. 2004). Minerals in the form of amino acid chelates have documented better bioavailability when compared with other forms of minerals. As an example, when an amino acid chelate of zinc was compared with zinc gluconate, the amino acid chelate increased the bioavailability of zinc by 43.4% (Gandia P, et al. 2007).
Magnesium, copper, zinc, and manganese are included in the BMJ as patented amino acid chelates.
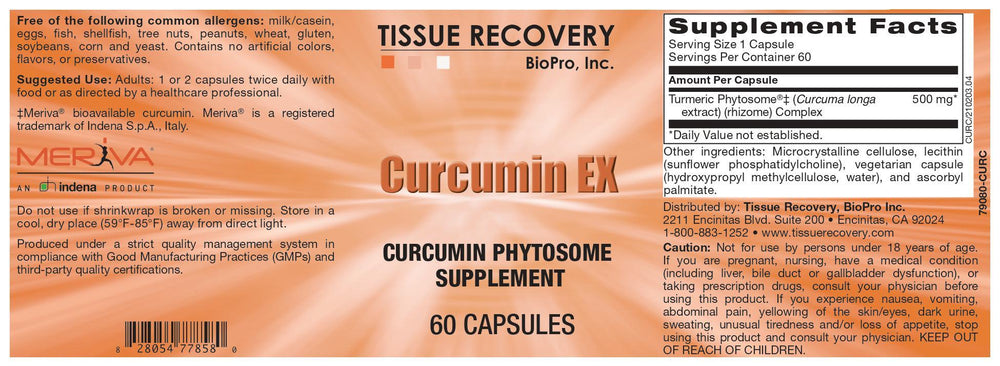
Vitamin D is important for many reasons and it is very common to be deficient or marginally deficient in this vitamin. Vitamin D has been documented to reduce the fracture risk in elderly persons (Bischoff-Ferrari HA, et al. 2009, Bischoff-Ferrari HA, et al. 2005). Vitamin D3 (cholecalciferol) is more efficient in sustaining vitamin D levels. Vitamin D2 potency is less than one-third of vitamin D3 and has a much shorter duration of action compared to vitamin D3 (Armas LA, et al. 2004).
Joints The BMJ contains 1500 mg of glucosamine sulfate in a daily serving which numerous studies have shown to be safe and effective in decreasing osteoarthritis pain (Reginster JY, et al. 2001, Pavelka K, et al. 2002, da Camara CC, et al. 1998, Foster PK, et al. 1995, Pujalte JM, et al. 1980, Drovanti A, et al. 1980, D Ambrosio E, et al. 1981, Lopes VA, et al. 1982.)
The graph below shows research comparing glucosamine sulfate with Ibuprofen for eight weeks (Vaz AL. 1982).
After four weeks the glucosamine sulfate produced more pain relief than the Ibuprofen.
Two studies conducted over three years documented that cartilage degeneration stopped in the treatment group taking glucosamine sulfate while the control group experienced further degeneration (Reginster JY. 2001, Pavelka K, et al. 2002). Research has documented that glucosamine sulfate supplies cartilage with building materials. Glucosamine sulfate caused a significant stimulation of proteoglycan production by chondrocytes (cartilage cells) in samples obtained from human osteoarthritic cartilage (Basleer C, et al, 1998). Another study showed that the treatment of osteoarthritic chondrocytes with glucosamine sulfate resulted in an increased cell-mediated GAG (glycosaminoglycans) content (Dodge GR, Jimenez SA, 2003). GAG is a common building block both for cartilage, ligaments, and tendons. Free radicals are also a factor involved in cartilage degeneration. Patients with osteoarthritis had approximately a four-fold lower level of extracellular SOD, the body owns antioxidant enzymes a constituent of cartilage (Regan E, et al. 2005). Zinc, copper, and manganese are necessary for the formation of SOD. That is one of the reasons these minerals are included in the BMJ. Vitamin D is also important for joints. An increased risk for osteoarthritis of the hip and knee has been documented in people with low-risk levels of vitamin D (Bergink AP, et al. 2009, Lane NE, et al. 1999). Osteoarthritis of the knee and hip progress more rapidly in patients with low vitamin D (McAlindon TE, et al. 1996, Lane NE, et al. 1999). A high percentage of patients with non-traumatic persistent, musculoskeletal pain have been found to be vitamin D deficient (Plotnikoff GA, et al. 2003). Research also shows that support of bone metabolism is important for cartilage integrity. Higher baseline serum osteocalcin, a marker of bone metabolism, has been found to be associated with a decreased rate of cartilage loss (Wang Y, et al. 2005). The BMJ includes important nutrients for both bone and joint metabolism. Vitamin B6 is included in the BMJ because it has shown to help prevent kidney stones when taken with magnesium (Prien E, et al. 1974, Gershoffs, et al. 1967).
The BMJ is now in Vegetable Capsules!
Suggested Use: Take 8 capsules in divided doses daily.
I've been using BMJ for several years. I decided to stop to make sure it was actually working. I found out quickly how well it worked. My joints were suddenly very achy. I'm very active and I won't try that experiment again.
j
janet Gilman Olson
A must-have supplement
This is the supplement that I never miss, along with glutathione. It contains all I need to fuel my body with essential nutrients to keep me active and agile.